
INTRODUCTION
Ossifying fibroma occurs mostly in craniofacialbones and categorized into two types central andperipheral. The central type of ossifying fibromaarises from the endosteum or the periodontalligament adjacent to the root apex and expands fromthe medullary cavity of the bone, and the peripheraltype occurs on the soft tissues overlying the alveolarprocess.1 Ossifying fibroma is a benign neoplasmcomposed of proliferating fibroblasts with osseousproducts that include bone and ovoid calcifications;and the lesions are well demarcated from theadjacent bone.
Many types of localized reactive lesions mayoccur on the gingiva, including focal fibroushyperplasia, pyogenic granuloma, peripheral giantcell granuloma and peripheral cemento-ossifyingfibroma (PCOF).2 It is widely considered that PCOForiginates from the cells of the periodontal ligament, and is often associated with trauma or local irritants, such as subgingival calculas, plaque, poor-qualitydental restorations and dental appliances.3Clinically, PCOF’s are sessile or pedunculated, withulcerated, and erythematous. Most lesions are lessthan 2 cm in size, although larger ones occasionallyoccur.3 It is more commonly seen in the first andsecond decades of life and has a femalepreponderance. There is a slight predilection for themaxillary arch (60%) and the incisor cuspid region(50%).4 The present case report comprised a growththat occurred in a 12 year old male child in themandibular anterior region which was diagnosed asPCOF.
CASE REPORT
A 12 year old male child reported with a chiefcomplaint of growth on lower teeth gums of anteriorregion since two months. On intra oral examinationa well defined solitary sessile growth of size 1x1 cmwas seen at interdental papilla in relation to 31 and41. The lesion was extending anterio posteriorlyfrom distal third of 31 to middle third of 41; andsuperio inferiorly from occulsal plane to attachedgingiva of 31and 41 (Figure 1). The lesion was alsoextending to lingual side through inter-dental gapof 31 and 41 (Figure 2). The lesion was soft inconsistency tender on palpation with bleeding onprobing.

|
Figure 1: Clinical photograph showing solitary sessile growth of size 1x1 cm at inter-dental papilla of 31 and 41.
Click here to view |

|
Figure 2: Clinical photograph showing lesion extending lingually through interdental gap of 31 and 41.
Click here to view |
Patient was advised routine hematological andradiographic investigations, where bloodinvestigations were with in the normal range andno significant changes were observed in theradiograph. Based on these clinical and radiographicfindings provisional diagnosis was made as pyogenicgranuloma.
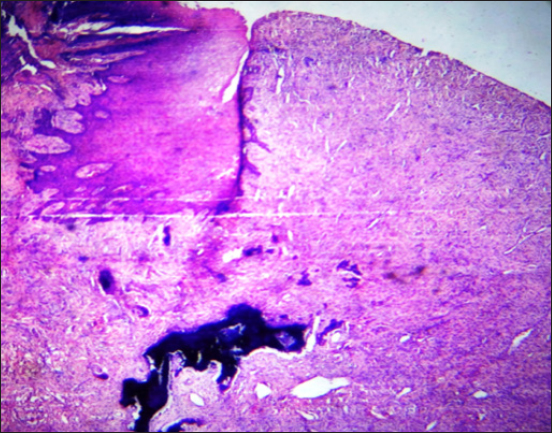
Under local anesthesia, the whole growth wasexcised and sent for histopathological examination. Sections were stained with routine H and E. Microscopic examination revealed hyperplasticparakeratotic stratified squamous epithelium ofvariable thickness (Figure 3). The underlyingconnective tissue stroma comprised of chronicinflammatory cell infiltrate and irregularmineralization foci (Figure 4) along with numerousspindle shaped fibroblasts. The cells were arrangedin a circular shape around irregular mineralizationfoci . The calcified areas resembled cementum-likeand bone-like ossifying areas (Figure 5). Clinicalassessment and histopathologic report confirmed thediagnosis as peripheral cement-ossifying fibroma(PCOF).
|
Figure 3: H and E stained section showing hyperplastic parakeratotic stratified squamous epithelium with variable thickness (x4).
Click here to view |
|
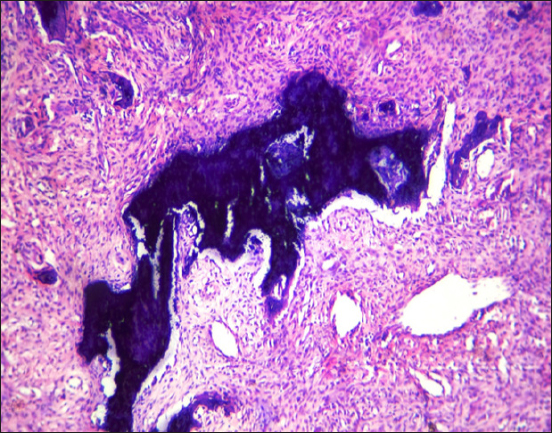
Figure 4: H and E stained section showing chronic inflammatory cell infiltrate and irregular mineralization foci (x10).
Click here to view |
|
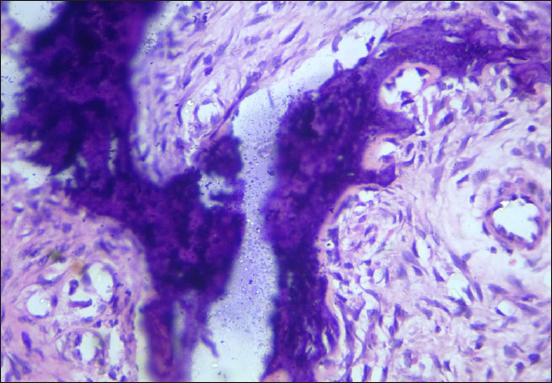
Figure 5: H and E stained section showing fibroblasts arranged in a circular shape around irregularmineralization foci . The calcified areas resemble cementum-like and bone-like ossifying areas (x40).
Click here to view |
DISCUSSION
Peripheral Ossifying Firoma (POF) was firstreported by the Shepherd in 1844 as alveolarexostosis. Menzel first described the lesion ossifyingfibroma in 1872, but its terminology was given byMontgomery in 1927.5 Eversol and Robin in 1972, later coined the term peripheral ossifying fibroma.2Peripheral-Ossifying Fibroma is a non-neoplasticreactive growth usually arise from the interdentalpapilla of gingiva. Various nomenclature are givenfor the POF by different authors, such as peripheralcementifying fibroma, ossifying fibro-epithelialpolyp, peripheral fibroma with cementogenesis, peripheral fibroma with osteogenesis, peripheralfibroma with calcification, calcifying fibroblasticgranuloma and calcifying or ossifying fibrousepulis.2, 6 When bone predominates the term’Ossifying’ is used and when curvilinear trabeculaeor spheroidal calcifications are seen the term’cementifying’ is used and when bone and cementum-like tissues are observed, the lesions have beenreferred to as cemento-ossifying fibroma innomenclature.7
Microscopic examination of H and E stainedsection reveals stratified squamous epithelium ofvariable thickness with underlying connective tissuestroma comprising of irregular mineralization focialong with numerous spindle shaped fibroblasts. Thecells will be arranged in a circular shape aroundirregular mineralization foci and the calcified areasresemble cementum-like and bone-like ossifyingareas. The present case report also confirms thepresence of irregular mineralization foci along withnumerous spindle shaped fibroblasts. The cells werearranged around irregular mineralization foci andthe calcified areas resemble cementum-like andbone-like ossifying areasdiagnosis as peripheralcement-ossifying fibroma (PCOF).
It is a fairly common lesion, comprising nearly3% of oral lesions. The site of occurrence of POF isusually anterior to molars in both maxilla andmandible equally, and in more than 50% of cases inthe incisor, and canine regions.2 The POF has a peakincidence in young and teenaged females. Cundiffreported that the lesion is prevalent between ages of 5 and 25 years, with a peak incidence at 13 yearsof age and he also reported a definite femalepredilection. Female to male ratio may vary from2:1 to 3:2.2 Excessive proliferation of mature fibrousconnective tissue is a response to gingival injury, gingival irritation, subgingival calculus or a foreignbody in the gingival sulcus.
Two schools of thought exist regardinghistogenesis of POF which are controversial:
-
1) POF may initially develop as pyogenicgranuloma that undergoes subsequent fibrousmaturation and calcification. It represents theprogressive stage of the same spectrum ofpathogenesis.
-
2) POF is due to inflammatory hyperplasia ofcells of periodontal ligament/periosteum. Metaplasiaof the connective tissue leads to dystrophiccalcification and bone formation.8
Lesions involving the gingival soft tissues arerare when compared to the lesions appearing withinbone. Mesquita RA found higher numbers ofArgyrophilic Nucleolar Organizer Regions(AgNORs) and proliferating cell nuclear antigen(PCNA)-positive cells in ossifying fibroma than inperipheral ossifying fibroma indicating higherproliferative activity in ossifying fibroma, X-raydiffraction analysis indicated that the mineral phaseof both central and peripheral tissues consists ofapatite crystals and that the crystallinity of theseapatites is lower than that of bone apatite. It wasalso suggested that the crystallinity of the apatitesmight improve progressively with the developmentof the lesion, possibly to the same degree as that ofbone apatite.9
An attempt has been made by Endo et al. todistinguish cementifying fibromas from ossifyingfibromas and fibrous dysplasias by usingimmunohistochemical analysis for keratan sulfateand chondroitin-4-sulfate, in which the cementifyingfibromas showed significant immuno-reactivity forkeratan sulfate, and ossifying fibromas and fibrousdysplasias showed intensive immunostaining forchondroitin-4-sulfate.7
CONCLUSION
PCOF is a slowly progressive lesion with limitedgrowth exclusively occurring on gingiva.7 Clinically, it is difficult to differentiate between most of thereactive gingival lesions particularly in the initialstages. It is important to eliminate the etiologicalfactors and the tissue has to be histopathologicallyexamined for accurate diagnosis and management. Treatment suggests surgical excision, including theperiosteum and scaling of adjacent teeth.7, 8