
INTRODUCTION
Tooth loss in the maxillary anterior region is the most psychologically traumatizing experience for the patient. It compromises the individual’s cosmetics and phonetics. Reassuring the patient and aesthetic rehabilitation of such regions are the most challenging conditions for the dental surgeon. Dental implants have become the preferred modality for prosthetic rehabilitation especially in such cases.
The conventional implant placement protocol requires 3-4 months of time for the consolidation of the tooth socket post extraction followed by surgical implant placement. An additional 4-6 months of time for osseointegration of these implants followed by functional loading.1 The entire procedure till the final prosthesis takes almost a year and the patient has to be left without a tooth/teeth for a prolonged duration.
To overcome the shortfalls of the conventional implant protocol especially the duration of treatment period, immediate implant placement into the extraction socket followed by early loading have become more popular. This protocol has several other advantages apart from reducing the treatment time. It preserves the alveolar bone and the gingival architecture to a great extent, fewer number of surgical procedures and so causes less amount of trauma. Thus this modality is well accepted by the patients as well.
CASE REPORT
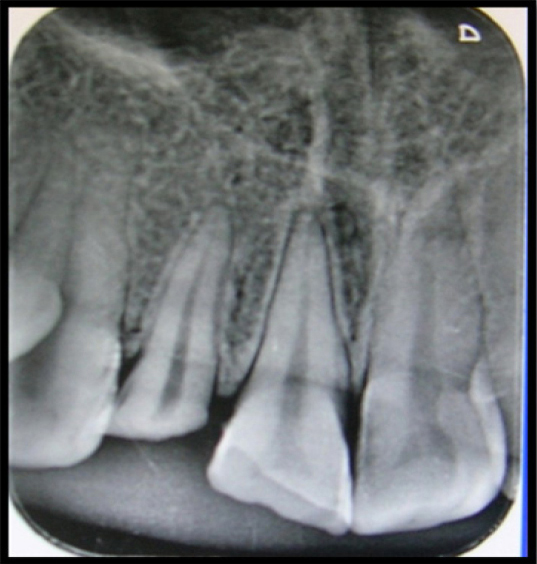
A 25 year old male patient reported to our dental centre with a history of trauma to upper front region of the jaw and fractured upper right central incisor. The intraoral clinical and radiographical examination revealed a fractured 11 and 12. 11 had a crown fracture involving the pulp and 12 with the fracture line running up to the cervical one-third of the root length (Figure 1 and 2). On consulting the endodontist, the fractured tooth did not have a good prognosis for reattachment procedure nor a good case for post retained crown. So, the treatment plan was formulated for endodontic treatment of 11 and extraction of root stump 12 followed by immediate implant placement into the fresh extraction socket and early loading. The procedure was explained to the patient and informed consent was obtained.

|
Figure 1: Pre-treatment clinical view showing fractured 11 and 12.
Click here to view |
|
Figure 2: Pre-treatment radiographic view showing fractured 11,12
Click here to view |
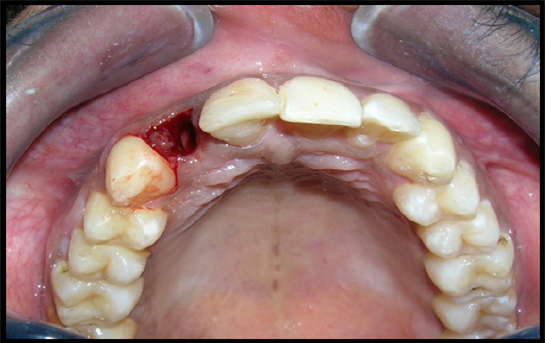
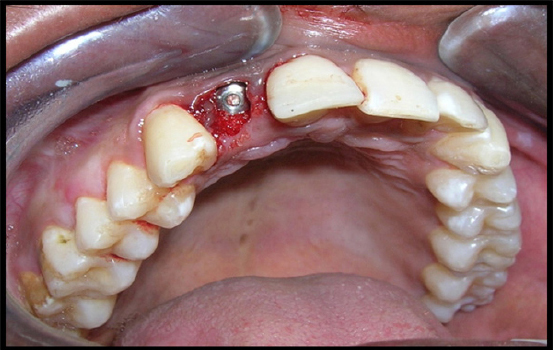
After administration of LA, mucoperiosteal flap was elevated and the extraction was performed as atraumatically as possible (Figure 3), careful examination of the socket was done and an implant of suitable dimension was placed into the fresh extraction socket, adequate primary stability was achieved and the wedge shaped space on the labial aspect of the implant was filled with perioglass alloplastic bone substitute (Figure 4) and the flap was approximated and sutured (Figure 5) and patient was prescribed analgesics and antibiotics. Final restorations were provided for 11 and 12, 8 weeks after the implant placement (Figure 6).
|
Figure 3: Extraction socket of 12.
Click here to view |
|
Figure 4: Immediate implant placement into the fresh extraction socket
Click here to view |

|
Figure 5: Clinical picture showing final implant prosthesis.
Click here to view |

|
Figure 6: Radiograph showing final implant prosthesis.
Click here to view |
DISCUSSION
The working definition for an immediate endosseous implant is extraction of a natural tooth followed by immediate placement of endosseous implant into the extraction socket in the same surgical procedure. Immediate implants are widely accepted and the available evidence suggests good levels of success. In general, the case selection criteria are based on the individual patient and focus on achieving predictable osseointegration, maximizing esthetic results, soft tissue maintenance and restoring function. The decision for extraction of teeth and replacing them with immediate implants is determined by a number of factors such as extensive carious lesion, periodontal attachment loss, unfavorable crown-to-root ratios, extensively restored teeth, loose endodontic posts, trauma, root fracture, root resorption, endodontic lesion and various combinations of the above. These factors ultimately affect the overall treatment plan.2 The number of remaining osseous walls is an important parameter, a minimum of 3-4 walls is essential for the success of immediate implants and violation of this results in significantly high implant failure rates. Also to be kept in mind is that a significant amount of alveolar ridge remodeling take place within 8 weeks following extraction, leading to a alteration of bone width and height on the facial aspect and a notable reduction in the width of alveolar crest.3, 4 The development of a mucosal recession after immediate implant placement may be because of the lack of a facial bone wall to support the facial soft tissues and a facial positioning of the implant.5 Primary stability is essentially the most important determinant for osseointegration because it allows for vital bone maintenance, clot stabilization, and prevention of soft tissue collapse and epithelial down-growth. The contraindications for immediate implant placement are presence of active infection, insufficient bone compromising the primary stability and extensive gingival recession. The esthetic requirements of single-implant treatment in the anterior maxilla represent an additional challenge.
The desired prosthetic outcome of immediate implant placement and early loading should display an implant-supported restoration surrounded by a soft and hard tissue environment in harmony with the existing dentition. In this context, the dental surgeon should work out on all the factors, surgical and prosthetic, that affect the final outcome. Inappropriate implant positioning or soft tissue management may lead to an esthetic disaster.6 Careful diagnosis and case selection are of utmost importance for a successful outcome. The current approach to immediate implant placement advocates palatal placement of the implant in the alveolar socket followed by placement of bone graft substitute in the resulting defect on the labial aspect of the implant to minimize esthetic failures due to soft tissue collapse or dehiscence.7 A systematic review in the year 2004 showed that the survival rates of immediate implants were comparable to implants placed in healed sites. However, the authors have stated that the clinical studies reporting esthetic outcomes of immediate implants in the anterior esthetic region are lacking in number.8
CONCLUSION
The ultimate goal of implant placement in the anterior esthetic zone is to reproduce the form and function of the tooth or teeth to be replaced. Keeping this fact in mind at all the stages of the treatment will improve the probabilities of a successful esthetic outcome. Immediate implant placement though highly acceptable by the patient, is considered a complex surgical procedure and should only be performed in after a thorough evaluation in selected patients.