
INTRODUCTION
The primary objective of endodontic therapy is the complete elimination of the bacteria from the infected root canal thereby preventing further re-infection. Unusual root canal morphology and presence of extra roots can pose a challenge to the clinician. Establishment of adequate access for thorough shaping and cleaning followed by three - dimensional obturation is crucial for the successful outcome of the treatment procedure. To achieve this, there is a need for an in- depth knowledge of root canal anatomy and its diversities such as extra roots, extra canals, webs, fins and isthmuses that may complicate the successful outcome of the root canal treatment.1
Mandibular molars are the most common teeth which are endodontically treated. Usually these teeth are known to have two canals in the mesial root and one or two canals in the distal root. Radix entomolaris is one of the anatomical variant seen in permanent mandibular molars and was first described by Carabelli. It is typically located on the disto-lingual aspect of first, second and third mandibular molar, occurring the least proportion in the second molar.2-4. Its presence is reported to vary significantly with races and ranges from 0 - 33.1%.5 It is known to occur in higher ratio among the population of Mongolian origin.
Though it is considered to be Asiatic trait with high prevalence among Chinese, Taiwanese and Koreans, found to be lesser in Indian population that is only 0.2%.6, 7 Various factors have been co-related with its occurrence such as gender, right verses left side distribution and bilateral incidence which are contradictory as there was no significant difference reported. Some studies have reported that there was about 37.14 to 67% of bilateral occurrence.8-10 When its presence is detected, proper diagnosis, identification and management of the additional root play a pivotal role in the endodontic success. The purpose of the present case report is to discuss the endodontic management of a radix entomolaris (RE) in mandibular second molar.
CASE REPORT
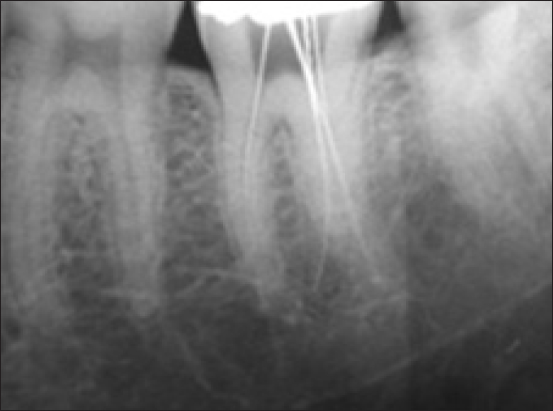
A 35- year old male patient was reported to the department of Conservative dentistry and Endodontics with the chief complaint of pain from past one week in left mandibular posterior region. The pain was lancinating type, severe, throbbing and continuous in nature and was aggravated by taking hot food and relieved by medication. Past medical history was non-contributory. On intraoral examination, a large deep occlusal carious lesion was seen in left mandibular second molar (#37). The tooth was asymptomatic to percussion and palpation. An exaggerated severe response was seen to cold and electric pulp tester. The mobility of the tooth was in physiological limits. Radiographic examination revealed deep carious lesion approximating the pulp and the presence of an extra distal root (Figure 1). The buccal object rule (same lingual opposite buccal rule) confirmed the additional root as a distolingual root (radix entomolaris). A diagnosis of acute irreversible pulpitis of 37 was established and endodontic treatment was planned. Informed consent was taken. After anaesthetizing the tooth using 2% lidocaine with 1:80,000 epinephrine, under rubber dam isolation, the carious lesion was removed and an adequate endodontic access preparation was done with endo-access bur and the canals were located. Upon pulpal floor examination, a dark line was observed between the distal orifice of the canal and distolingual corner of the pulp chamber floor. At this stage, the dentin was removed through diamond- coated ultrasonic tips (size TRA 24, Dental Trinks, Sao Paulo, SP, Brazil ) mounted in a ultrasonic device (Gnatus, Ribeirao Preto, SP, Brazil), and a second distal orifice of the canal was detected. The enlargement of the cervical and medium thirds through nickel-titanium rotary instruments (ProTaper Universal, sizes S1 and Sx, Dentsply Maillefer, Ballaigues, Switzerland) and Gates- Glidden burs (sizes 4, 3 and 2; Dentsply Maillefer, Ballaigues, Switzerland) was performed, resulting in more visible canals, including the radix entomolaris canal. The canal lengths were determined radio graphically with K file ISO 15 size and electronically with Root ZX (Figure 2). They were cleaned with 2.5% sodium hypochlorite along with EDTA and shaped with pro-taper rotary system till a size of F-2 and patient was recalled after 3 days. At next appointment patient was asymptomatic. Master cone radiograph revealed proper fitting of cones (Figure 3) .Canals were dried with paper point and obturation done by using zinc oxide eugenol sealer (Figure 4).

|
Figure 1: Radiograph showing pre-operative view of radix entomolaris in 37
Click here to view |
|
Figure 2: Radiograph showing working length determination.
Click here to view |

|
Figure 3: Master cone selection
Click here to view |

|
Figure 4: Post obturation radiograph
Click here to view |
DISCUSSION
Mandibular second molars usually have two roots and three root canals. However, variations from these have been reported in various studies.11 Presence of middle mesial canal and radix entomolaris can be attributed to such anatomical variants. An accurate diagnosis of these aberrant root and canal morphology helps in avoiding the complications like missed canal which is the most common reason for endodontic failure.
Thorough examination of the preoperative radiograph is mandatory to detect the existence of invisible RE by specific features such as unclear view or outline of the distal root shape. Two different radiographs are to be taken from a more mesial or distal angle in order to reveal its presence.12 After its identification, the access cavity preparation needs to be modified from a conventional triangular access to a rectangular or trapezoidal outline.13 It is made by the spread of the triangular opening cavity to the lingual. A dark line on the pulpal oor shows the accurate place of the RE canal aperture. Visual supports like a loupe, intra-oral camera or dental microscope are beneficial. Flexible nickel titanium files are helpful in the initial negotiation of the canal. Guide path should be created before the preparation which helps in the prevention of procedural errors. Finally, use of nickel-titanium rotary files having a taper of not more than 0.04 taper and crown down technique is said to allow a more centered, rounder and conservative canal preparation than the use of stainless steel instruments in RE.13-15
Thorough knowledge of such external and internal anatomical variations helps the clinician in diagnosis and management. Various diagnostic measures are important aids in the location of root canal orifices which include multiple radiographs, examining and staining the pulpal floor, performing champagne bubble test, troughing grooves with ultrasonic tips. In the modern era, newer techniques like use of CBCT, dental operating microscope, dental loupes are beneficial in the endodontic management of these teeth.
CONCLUSION
Failure to identify and detect the anatomical variations of the root canal system can significantly affect the outcome of the endodontic treatment. Though the angulated radiographs and recent imaging techniques, play an important role in the identification and endodontic management of these variations, the clinician should be aware of the prevalence, diagnosis, morphology, canal configuration and the clinical approach to treat such unusual root morphologies in mandibular molars which contribute to the successful endodontic therapy.
Conflict of Interest
There is no conflict of interest regarding the publication of this manuscript.