
Introduction
Fear and anxiety are two concepts that are closely associated and for which there are many definitions. Fear is a response to a specific stimulus while anxiety is a result of a more general or pervasive stimulus. Geer stated that the difference between fear and anxiety is thus conceptualized as a difference in the specificity of the stimulus.1 Corah stated that dental anxiety is more specific than general anxiety; it is the patient’s response to the stress specific to the dental situation.2 Dental anxiety is a topic of concern for professionals as it prevents many potential patients from seeking treatment and also causes strain to the dentists undertaking dental treatment. Hence it can be challenging for the dental practitioner to treat young children at their level of cooperation can be restricted because of their anxiety.3
Dental anxiety among 13-14 year-old children were investigated by Bedi et al who reported a prevalence of 7.1% with a higher level among girls and in children of lower socioeconomic classes.4 Dental anxiety is most commonly measured using questionnaires and behaviour rating scales.5 Many techniques have been augmented to manage the anxiety of children in dental clinics. However, according to the American Academy of Pediatric Dentistry conference in 2003 it was reported that there were more studies done on pharmacological management technique than that of non- pharmacologic techniques 6
Several studies have shown that Tell Show Do (non- pharmacological technical) is the most commonly used technique in pediatric dentistry. It consists of explaining and demonstrating the technique and the instruments used during treatment.6-9
Modelling another non- pharmacological technique is worth exploring. According to a review by Baghdadi, Modelling was described by Bandura in 1967, which is a course of acquiring behaviour of a model by observing.10 The first study of Modelling in pediatric dentistry was conducted in 1969, which was reported by Greenbaum and Melammed, later several other studies followed in the 1980s.8, 11, 12
According to these literature studies, 2 forms of modelling, live and filmed, both are effective in decreasing children’s fear and anxiety about dental treatments and promote positive behaviour.11-15
According to the recommendations of the American Academy of Pediatric Dentistry on the need to study nonpharmacologic behaviour- management techniques by means of various clinical protocols, the present study was undertaken to compare the effects of filmed modelling and the Tell- show-do method on anxiety in children undergoing dental treatment based on their heart rates and modified venhams anxiety scale.16, 17
Materials and Methods
A randomized clinical trial study was done on 20 children aged between 6-9 year who reported to the Department of Pedodontics and Preventive Dentistry, College of Dental Sciences, Davangere, with the chief complaint of decayed teeth and who met the following inclusion & exclusion criterion were selected.
Inclusion Criteria
Children were eligible for the study if they presented for a first visit to the dental care centre, no medical history that might affect the heart rate and who had only occlusal caries (class I).
Exclusion Criteria
Teeth were excluded if there was a history of pain, abcess or there was definite or likely pulpal exposure. Informed consent was taken from parents of all participants prior to starting the treatment procedure.
The study subjects were randomly divided into 2 groups.
Group A: Ten Children were conditioned to receive dental treatment by Tell show do technique (TSD). It consists of explaining and demonstrating the procedure and the instruments used during treatment.6-9
Group B: Remaining Ten Children were conditioned for dental treatment by Filmed modelling (FM) technique with a video showing modelling by another child.13
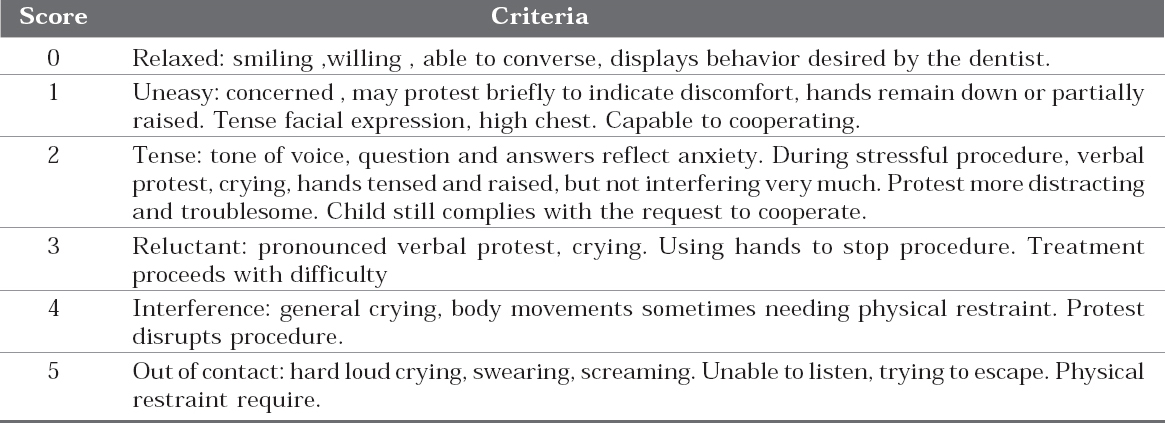
After conditioning each subject, class I cavity preparation was prepared using a high speed hand piece with water spray, later the teeth were restored with type II GIC under isolation using suction tip and cotton rolls. The anxiety level was recorded at 5 different stages during treatment using heart rate and Modified venham anxiety scale (Table 1)16,17
|
Table 1: Venham index (modified 6-point scale according to venham)16,17
Click here to view |
When the child was sitting in the waiting area
After demonstrating the behavior management technique. (Tell- Show-Do or Filmed Modelling)
After the completion of cavity preparation
At the moment when restoration was completed.
After the child was sent out of the operating room.
The heart rates of the patients were measured using a portable pulse oximeter device applied on the finger of the child. Both the recordings of the heart rate and the observations were carried out by one dentist, not taking part in the actual treatment of the children.
Statistical Analysis
To analyze a difference in the modified venham score between the two treatment groups, a chi square test was used. Student’s t- test was used to measure the heart rates of children recorded in both the treatment groups. Pearson’s correlation coefficient was used to assess the relation between the heart rate and venham score.
Results
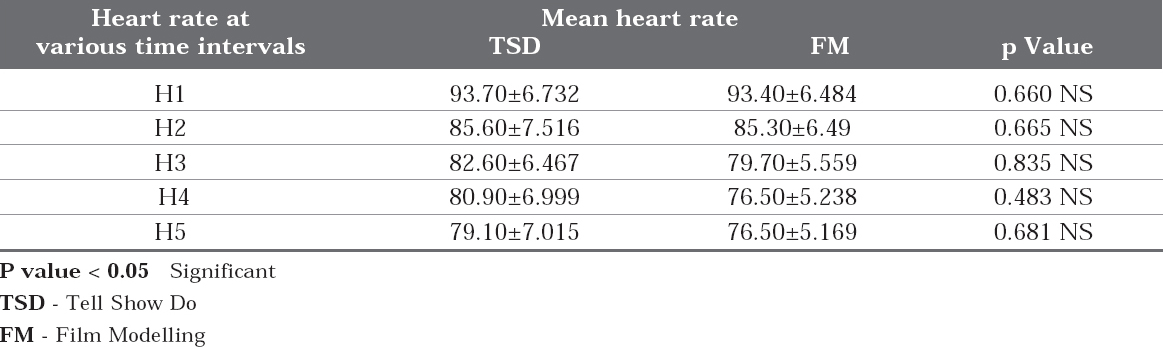
A total of 20 children aged 6-9 years participated in the study. The Table 2 shows Student’s t-test which was done to compare heart rate between Tell- Show-Do and Modelling group at various time intervals. The p-value for both the treatment groups at various time intervals were for Hj-0.660, H2-0.665, H3-0.835, H4-0.483 and H5-0.681 respectively. Student’s t-test shows that there was no significant difference in both the treatment groups, and there was a decrease in heart rate from H1 to H5 in both the treatment groups.
|
Table 2: Depicts Student’s t-test which was done to compare heart rate between 2 groups at various time intervals.
Click here to view |
Table 3: shows the distribution of the sample according to modified venham score at various time intervals of both the techniques. The p-value at the 1st interval was 0.767, 2nd interval 0.881, 3rd interval 0.565, 4th interval 0.587 and 5th interval 0.513 respectively. The result was statistically in significant indicating that there was a reduction in modified venham score from interval 1 to interval 5 in both the groups compared.

|
Table 3: Distribution of sample according to venham score at various time intervals of both the techniques
Click here to view |
And Table 4 shows Pearson’s correlation coefficient to measure the relation between the heart rate and modified venham score. This test shows that there is highly positive correlation observed at different time intervals, which means that as the heart rate increases the modified venham score also increases.

|
Table 4: Depicts Pearson’s correlation coefficient to measure relation between the heart rate and venham score.
Click here to view |
Discussion
Noise, vibration of the drill, the sight of the injection needle and sitting in the dental chair have been reported to cause fear and lead to unfavorable behaviour in children.18 Most often than none, fear of pain appears to be the most important predictor of dental anxiety. Dental fear is a multifactorial problem encountered during dental treatment which originates mainly in childhood, so it is important that these fears are addressed early.19 The role of the dentist is important in developing an understanding of how children become dentally fearful. Therefore the dentist should be capable to identify the children having dental anxiety, assess their fears and help them to build confidence to overcome those fears. Suitable behavior management techniques like behaviour shapping, Tell-Show-Do, and modelling should be instituted in children who are predicted to behave poorly during treatment.
Tell-Show-Do is a technique based on the principle of learning theory. Several epidemiologic studies have shown its positive effect on the reduction of dental anxiety, but, performance of Tell- Show-Do needs time constraints of both the dentist and the parents.20 Another technique is Modeling. Two forms of modeling, live and filmed, have been found to be effective in reducing children’s fear and anxiety about dental treatments and promoting adaptive behaviours.11 According to several studies film modeling is proved to be efficient in reducing child’s dental anxiety.13, 21-23 It has been shown that Filmed modeling can be effective as well as live modeling and also desensitization methods.21, 23 Contrary to other behavior management techniques, Filmed modelling does not take much time by the dentist or his team; although it has not gained much attention.11
Thus the objective of this study was to compare Tell-Show-Do (TSD) technique and Filmed Modelling (FM) on anxiety in children undergoing dental treatment based on Children Heart Rates and Modified venhams anxiety scale.
In our study, Filmed Modelling was as efficient as TSD to reduce anxiety in children and gain cooperative behaviour during dental treatment. The results of our study coincide with the studies done by various authors, Machen and Johnson and Melamed et al who have found the effectiveness of Filmed Modelling in comparison to desensitization in various patients.21, 22
A study done by Prayab and Hosseinbor M et al reported that high prevalence of severe dental anxiety may be seen in the early years of school.24 However, general factors like family factor is seen to have less influence on the behaviour of a school aged child during a dental visit. So the school children of age group 6-9 years were taken in our study so that we could demonstrate proper behaviour management technique and which could help us in assessing the reduction in their dental anxiety.
Various researchers have investigated fear and anxiety in children using different scales and measurements.25-27 Modified 6-point Venham Index was used in the study whose validity and reliability has been substantiated by Veerkamp JSJ and Nathan JE et al.28, 29 In our study anxiety and behavioral levels were assessed by two indexes (Physiological and Behavioural indexes). The physiological index was assessed by heart rate using pulse oximeter. Heart rate measurement related to dental anxiety has been researched and found to be positively related to each other.30 The measurement tool used in the present study was pulse oximeter which is considered as an excellent means of monitoring heart rate, portable finger pulse oximeter, which itself will be less anxiety provoking in children. In our present study positive correlation was established between heart rates and Modified venham score at all five intervals of measurements which coincides with the study done by Roshan et al.16
Heart rates of children in our study for both the treatment groups in the waiting area were higher (TSD 93.70±6.732, FM 93.40±6.484) which was similar to previously mentioned study and after doing behavior management by either TSD and FM the heart rates reduced (85.60±7.516 and 85.30±6.49) which was statistically not significant.16 This finding coincides with the study done by Paryab et al.17 Although the result in both the treatment groups was statistically not significant, but we could see that there was a decrease in heart rate and improvement in behavior from H1 to H5 interval in both the groups.
Gender is thought to be one of the factor which may influence the anxiety levels in children. Previous studies states that fear and anxiety are related to gender difference.31 The results of our study for a given age group shows that anxiety level was similar in both boys and girls, which coincides with previously mentioned study.16 This finding is in contrast to the study done by Schricks MCM and Van Amerongen WE who have reported more anxiety for dental procedures in girls than in boys.30
It is of utmost importance to give much attention to every child on their visit to the dental clinic and perform simple behaviour management techniques that can create a profound effect in achieving our goal to teach good oral health and positive approach towards dentistry. Parental acceptance of behavior management technique used by a pediatric dentist is another concern. Parents reported a significant preference for non invasive reinforcement techniques instead of sedation and restraints.32 In the present study both TSD & FM behaviour management techniques were effective in reducing child’s fear and anxiety as most of the children in our study were showing cooperative behavior at the end of the treatment. Hence the behaviour management techniques should be such that the child eagerly returns for the treatment and follow up at regular intervals of time throughout his lifetime and carry a positive approach towards dentistry .
Conclusion
Assessment of behaviour is the most important tool in the hands of the dentist. This helps the dentist to execute the required treatment plan in the most appropriate manner in children. Based on our study results, Film modelling was as effective as Tell- Show-Do technique so it can be used as an alternative to Tell-Show-Do technique and both behaviour management techniques (i,e) Tell-Show- Do and Filmed Modelling are effective in reducing child’s anxiety levels who are undergoing dental treatment. However, the limitation of the present study is modelling and Tell-Show-Do were compared for a particular treatment (restoration) only. Future research comparing all possible treatment after film modelling with Tell-Show-Do would give better insight about the efficacy and effectiveness of above mentioned behaviour management techniques.