
Introduction
Tooth development results from a complicated multistep interaction between the oral epithelium and the underlying mesenchymal tissue. A series of complex tissue interactions result in the formation of mature teeth. Abnormal tissue interactions during tooth development may potentially result in ectopic tooth development and eruption.1, 2 The dentigerous cyst is a developmental odontogenic cyst which originates through alternations of the reduced enamel epithelium in an unerupted tooth, after the crown has been fully formed.3Most commonly mandibular third molars, other common associations are with maxillary third molars, maxillary canines, and mandibular second premolars. They may also occur around supernumerary teeth and in association with odontomas.4, 5 Ectopic tooth erupting into maxillary sinus is usually rare with few cases in literature. Ectopic eruption may result due to one of the following three processes: developmental disturbance, pathological process and iatrogenic activity.6 Here we present a case with dentigerous cyst involving left maxillary antrum with impacted third molar which was treated under general anaesthesia by approaching lateral window technique and closure done with buccal fat pad.
Case Report
A 27 years old female patient reported with a complaint of discomfort and heaviness in left maxillary tooth region since 6 moths. History revealed that she has used medication for the same but symptoms didn’t resolved. Extraorally, no inflammatory changes are seen on left maxillary region Intraoral examination showed missing left upper third molar and partially erupted bilateral lower third molars. No obliteration of buccal vestibule or no signs of swelling on palatal side.Panaromic radiograph showed third molar in upper left maxillary sinus (Figure 1). On CT examination axial, coronal and sagittal CT images showing impacted third molar in the posterior aspect of left maxillary sinus (Figure 2).
s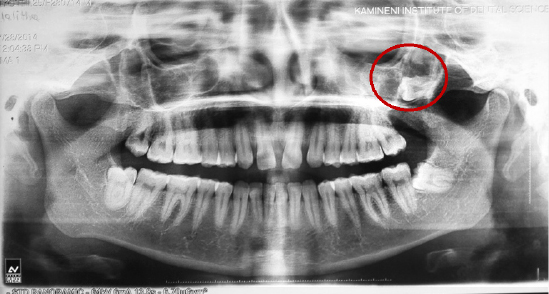
|
Figure 1 : Pre-operative panaromic radiograph showing impacted third molar in the left maxillary sinus.
Click here to view |

|
Figure 2 : Axial, coronal and sagittal CT image showing impacted third molar in the posterolateral aspect of left maxillary sinus
Click here to view |
After performing routine surgical profile screening cyst enucleation along with defect closure using buccal fat pad is planned under general anaesthesia. A full thickness mucoperiosteal flap reflected from left maxillary second premolar to second molar. A 2 cm window was created in the lateral wall of maxilla and necrotic mass was curetted out. Along with the impacted third molar cystic lining was removed (Figure 3) and sent for histopathological examination. After enucleation buccal fat pad was teasedout carefully from same incision extending posteriorly and brought in to the surgical defect with the help of artery forceps (Figure 4). Care must be taken not to damage the buccal fat pad and its blood supply. Buccal fat padsecured in position with the help of 4 - 0 vicryl then mucoperiosteal flap is replaced to its original position to prevent any loss of buccal vestibule (Figure 5).

|
Figure 3 : Excisional biopsy specimen showing cystic lining with tooth
Click here to view |
|
Figure 4 : Buccal fat pad placed into the bony window
Click here to view |

|
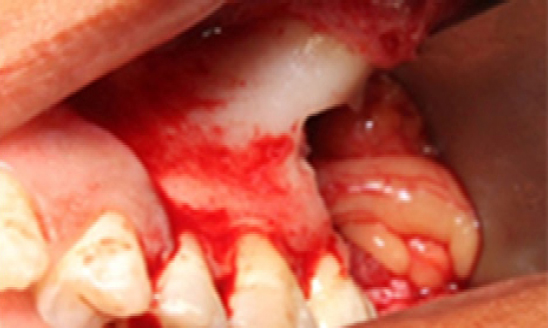
Figure 5 : Intra oral picture showing closure of the defect
Click here to view |
Post operatively healing was uneventful without any complications and patient has no complain of discomfort or heaviness even after a follow-up period of 2 years. Panaromic radiograph shows good bone healing at the operated site.
Discussion
Eruption of teeth into regions other than the oral cavity is rare, although there have been reports of teeth in the nasal cavity, mandibular condyle, coronoid process, and palate.2, 7 One of the sites for an ectopic tooth in a nondental location is the maxillary sinus.2, 8 They usually present with local sino-nasal symptoms attributed to recurrent or chronic sinusitis. The diagnosis and treatment plan of this condition can be made radiographically by OPG along with CT scans taken in all sections.1
Dentigerous cyst is the most common of all follicular cysts, more common in males, occurring in the second or third decade of life. About 70% of dentigerous cysts occur in the mandible and 30% in the maxilla.9If infected, the treatment of choice is complete enucleation of the lesion intraorally with removal of the associated tooth. It is also important to completely remove all diseased antral tissues and thoroughly assess all resected soft tissue histologically with a follow-up for a period of 1 year.10 Pedicled buccal fat pad flaps have been recommended for the closure of fistulas and in various areas; the use of pedicled buccal fat pad flaps has also been employed in the resolution of unsuccessful surgical cases in which lesions have developed. Among the advantages of this technique are the low morbidity rate, maintenance of the vestibular sulcus depth, the low incidence of failure, and the good flap vascularization.11
The standard treatment for a dentigerous cyst of maxilla is enucleation and extraction of the associated tooth via a Caldwell Luc procedure under local or general anesthesia. In large cysts, an initial marsupialization to diminish the size of the osseous defect, followed by enucleation and tooth extraction, has been followed. The major disadvantage of marsupialization is recurrence or persistence of the lesion along with the residual cystic lining. Endoscopic approach for management of dentigerous cyst of maxilla is also described in the literature. This method is associated with lesser operative as well as postoperative morbidity.14 Dentigerous cyst of maxilla may cause pathological jaw fracture if large enough, may transform into ameloblastoma, and has the potential of developing into squamous cell carcinoma and mucoepidermoid carcinoma if there is chronic infection. It has a recurrence rate of about 12-14%.1315
Conclusion
Dentigerous cyst involving maxillary sinus with ectopic third molar is rare entity. At initial stage dentigerous cyst involving maxillary sinus present asymptomatic unless it gets infected. Use of orthopantomograph and CT scan can help diagnosing the lesion and appropriate treatment planning. Treatment of such lesions by enucleation along with removal of tooth involved has to be indicated. Untreated cases of dentigerous cyst can undergo malignant transformation. Closure with buccal fat pad after enucleation of dentigerous cyst with third molar found to be a superior.