
INTRODUCTION
Treatment of skeletal Class III malocclusion in growing patients is a challenging part of contemporary orthodontic practice. The etiology of skeletal Class III malocclusion is believed to be mainly hereditary, but environmental factors such as mouth breathing and habits may also play a role.[1,2] Multiple studies have documented that the prevalence of angle Class III malocclusion varies greatly within different geographic regions and races.[3]
Skeletal Class III malocclusion may result from: (1) Maxillary retrusion, (2) mandibular protrusion, or (3) combined maxillary retrusion and mandibular protrusion. McNamara and Ellis found that 65–67% of Class III malocclusions were characterized by maxillary retrusion.[4]
The timing of correction of skeletal Class III malocclusion is critical for optimum results. The typical age for a successful maxillary protraction treatment is said to be before the age of 10 years. Franchi et al. found that the greatest orthodontic effect was in the early mixed dentition (about the age of 8 years old) versus later stages in skeletal growth and dental. However, patients treated in late mixed dentition still benefited.[4-6]
Many appliances are now available for correcting skeletal Class III malocclusion due to maxillary deficiency. In 1970, popularized the concept of correcting maxillary protraction with face mask.[7] In 1983, modified the Delaire mask by increasing the amount of force generated by the appliance.[8]
Orthopedic treatment of Class III malocclusion has been described utilizing a Delaire, Petit style face mask, and reverse headgear for maxillary deficiency.[9] Many of the literature showed that many of the treatment approaches can be found in regarding orthodontic and orthopedic treatment of Class III malocclusion including reverse twin block, modified tandem appliance, and two-piece magnetic appliance.[10-12]
In the current study, the Wunderer’s activator and face mask were used for the correction of skeletal Class III in growing patients to overcome the latter side effects of these appliances. The research hypothesis assumed that no significant difference exists between the Wunderer’s activator with a face mask and other appliances.
MATERIALS AND METHODS
A total of 12 growing Class III patients were selected from the clinic of the orthodontic department, faculty of dentistry. The cases involved in this study had following criteria: (1) Early mixed or early permanent dentition at the start of treatment characterized by a wits appraisal of −1 mm or less, (2) skeletal Class III due to maxillary deficiency, (3) reverse overjet and reverse overbite, (4) no cleft and other craniofacial anomaly, and (5) no previous orthodontic treatment.
Control group was not taken in the present study for ethical purposes to avoid exposing the patient to extra radiation without the benefits of treatment. All orthodontic records were taken for every case. Lateral cephalograms, photography, and models were prepared before and after treatment changes produced by Wunderer’s activator and face mask.
The cases and their parents were informed about the study and the steps of treatment, and the parents signed consent forms. In addition, assent forms were required from the children who participated in the study.
For each patient, good upper and lower silicon rubber base impressions were taken and bite construction was registered using exactobite in the most retruded of position the mandible. The bite was transferred to the working upper and lower models, articulated in the hinge articulator and used for appliance fabrication.
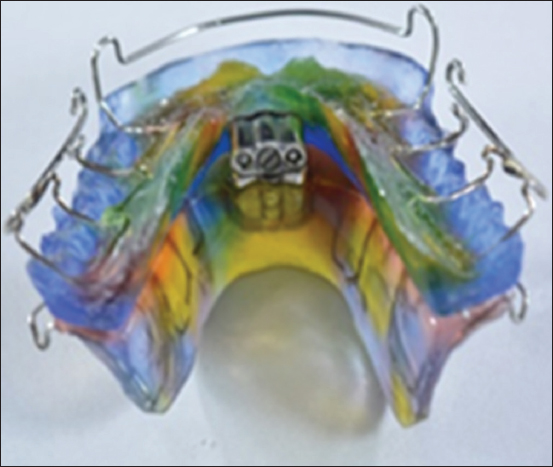
Wunderer’s activator is a removable appliance composed of Adams clasp made of 0.9 mm stainless steel (SS) wire on the permanent first molars and short labial bow made of 0.8 mm SS wire were constructed on anterior incisor teeth of both casts. All the components were waxed and a separating medium was applied to the upper and lower casts. The acrylic part was split horizontally with the upper and lower portions connected by Weise screw [Figure 1]. Part of the Weise screw was embedded in the mandibular portion of the activator and the other part of the screw was attached to the maxillary portion of the activator [Figure 2]. Acrylic base plate was made in the upper and lower casts to connect the components of the appliance with a posterior bite plane in between [Figure 3]. Wunderer’s activator had two hooks, one on each side in the upper area of the activator at the premolar areas roughly 15 mm gingival to OCPs for the attachment of elastics [Figure 4], trimming and polishing of the appliance were done to finish it [Figure 5].

|
Figure 1: Weise screw
Click here to view |

|
Figure 2: Screw is attached to the maxillary portion of the activator
Click here to view |

|
Figure 3: Acrylic base plate was made in the upper and lower casts to connect the components of the appliance with a posterior bite plane in between
Click here to view |

|
Figure 4: Two hooks one on each side of the upper part of Wunderer’s activator, roughly 15 mm gingival to occlusal planes for the attachment of elastics
Click here to view |
|
Figure 5: Wunderer’s activator
Click here to view |
Face mask
Delaire type face mask was attached to the hooks of Wunderer’s activator. The face mask was inserted [Figure 6], and an orthopedic force of at least 500 g per side directed 30° downward and forward from the OCP was applied by heavy extraoral elastics (Ormco, Orange, Calif). The force was measured by a force gauge (Correx Tension Gauge; Haag-Streit Diagnostics, Koeniz, Switzerland). Instructions during the study period: The patients included in the study were instructed to wear the device for a minimum 14 h every day including the sleeping time. Intraoral appliance had to be removed and cleaned with normal water and mouth cleaning every day to avoid bad odor.

|
Figure 6: Delaire face mask
Click here to view |
Follow-up was done every 3 weeks, but if there was damage of any part of the appliance or it became unfitted, back directly to the clinic should be done. The elastics were changed every day. Activation of the appliance was achieved by turning the screw using the screwdrivers 1/4 turn twice a week.
All cephalometric radiographs were scanned and analyzed by one investigator using Dolphin Software (Version 11.7; Dolphin Imaging and Management Solutions, Chatsworth, Calif). The analysis consisted of the following:
Angular measurements (sympathetic nerve activity [SNA], sella-nasion B [SNB], ANB, SN/OCP, SN/GoGn, SN-U1, U1-NA, U1-palatal plane, L1-NB, L1 mandibular plane [MP], U6-SN, U6-PP, and U6-MP) and linear measures (U1-NA, L1-NB) [Figure 7].

|
Figure 7: Linear and angular cephalometric measurements
Click here to view |
After correction of the overbite and overjet, the appliance acted as a retainer. After growth modification, correction to start the second phases of treatment for relief any dental malocclusion.
Statistical analysis
Date from cephalometric radiographs was examined using IBM SPSS Program Version 20.0 90. Quantitative data were described using standard deviation, mean and after testing normality using Shapiro–Wilk test. Significance of the obtained results was judged at the 5% level and highly statistically significant at P < 0.01. The used tests were paired t-test for quantitative parametric variable, to compare between before and after treatment measures with calculation of mean difference by subtracting post-treatment results minus pre-treatment results.
RESULT
A total of 12 participiates of both genders (six boys and six girls of the sample) used the Wunderer’s activator and a face mask with average age of 8.50 ± 2.35 years. The data in Table 1 showed that the SNA angle was highly significant increased by 1.98°. Anterior movement of a point was confirmed by the highly statistically significant increase of the ANB angle by 2.86° (P < 0.001). Furthermore, the wits appraisal was found to be highly significant increased by 2.8 mm. On the other hand, statistically significant decrease in the SNB angle was detected by −0.83° (P < 0.001). Regarding the vertical results in the present study showed significant increase in SN-OCP and SN- Gonion-Gnathion (GOGN) by 2.01° and 1.75°, respectively. Regarding the linear and angular dentoalveolar changes in this work, the maxillary incisors proclination was highly significant increased and mandibular incisors inclination was significantly decreased. The U1/NA, L1/NB, U1-SN, U1/pp, and L1/MP recorded (p <0.007, 0.28, 0.02, 0.046, and 0.007, respectively). The U6/SN, U6/PP, and L6/MP lines were not significantly affected.

|
Table 1: The present study showed the following linear and angular cephalometric measurements
Click here to view |
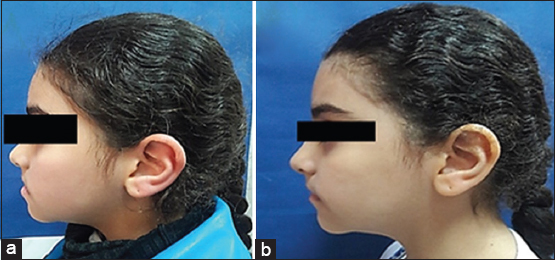
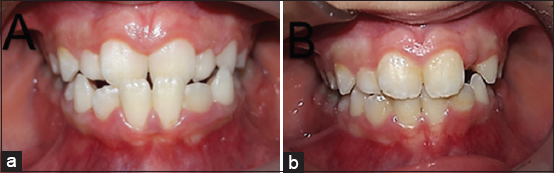
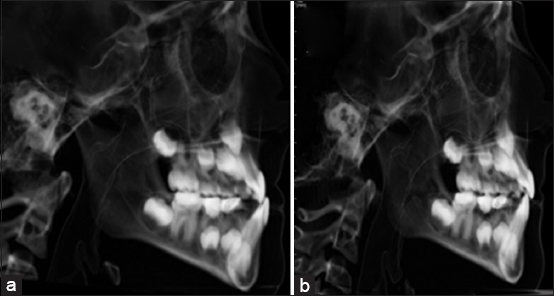
A case treated by face mask and Wunderer’s activator, extraoral view pretreatment and post-treatment [Figures 8 and b], intraoral view before and after treatment [Figures 9a and b], and cephalograms view before and after treatment [Figures 10a and b].
|
Figure 8: Extraoral profile views: (a) Before face mask and Wunderer’s activator; (b) after face mask and Wunderer’s activator
Click here to view |
|
Figure 9: Intraoral profile views: (a) Before face mask and Wunderer’s activator; (b) after face mask and Wunderer’s activator
Click here to view |
|
Figure 10: Cephalograms view: (a) Before face mask and Wunderer’s activator. (b) After face mask and Wunderer’s activator
Click here to view |
DISCUSSION
Skeletal Class III malocclusion can be manifested as maxillary retrognathism, mandibular prognathism, or a combination of both. “To or not to” intervene is a common dilemma faced by orthodontists and pediatric dentists when confronted with a developing Class III malocclusion. Correction of skeletal Class III malocclusion was thus initiated in the early transitional dentition to have maximum skeletal effects according to McNamara.[13] Many appliances were used to treat skeletal Class III malocclusion.[14,15] The present work was conducted to evaluate the effects of one of these appliances which is Wunderer activator with a face mask.
In this study, the Wunderer’s activator and face mask were efficient in the correction of skeletal Class III malocclusion due to maxillary retrusion with the slight increase in vertical dimension and they improved the skeletal intermaxillary discrepancy. The results of the current study showed that Wunderer’s activator with face mask can efficiently improve the dentoskeletal of patients with maxillary retrusion.
Regarding the skeletal anteroposterior effects, the results showed significant increase in the SNA angle were found. This was due to the use of face mask which provided direct constant anterior force to the maxilla, leading to anterior displacement of the maxillary sutures. The Wunderer’s activator served as an intraoral appliance for the attachment of force modules as well as it created anterior force on the maxillary arch. Increase in the SNA angle was approved by McNamara, Tortop et al.; in contrast to the results of Ulgen and Firatli who utilized the Frankel III appliance had no effect on the SNA.[14-17] Decrease the SNB angle was due to more backward displacement of the mandible with rotation, this might have been due to the chincap effect of the face mask therapy. This explains the slight increase in the facial height, also the mandible was held in the most retrusive position during treatment, this retrusive position led to forward and downward motion of the maxilla while mandible moved downward and backward. Thus, the ANB angle increased significantly due to the anterior movement of A point and posterior movement of B point. This outcome was in agreement with those of Arslan et al, McNamara, and Altug and Arslan.[14,18,19] On the other hand, this result was in contrary to study conducted by Mermigos et al. and Kulbersh et al., where the ANB angle was increased by the increase in the SNA angle only.[20,21] Regarding the vertical dimension in the current study, there was revealed slight increase in SN/OCP and SN/GOGN, respectively, this could be due to the rotation of the mandible; this might have been due to the chincap effect of the face mask therapy.[22] The effects of the face mask are a combination of dental and skeletal changes in the mandible and the maxilla. The maxilla moved downward and forward as a result of the protractive force. As a consequence of this effect, the mandible rotated downward and backward, thus improving maxilla-mandibular relationship in the sagittal dimension. However, this led to increase in the lower facial height, also the vertical dimension can be managed in hyperdivergent growth patients by utilizing appliances with interocclusal acrylic, Wunderer activator had it, Dorothea Dausch-Neumann, Tubingen.[23,24] Results of dentoalveolar changes were highly significant increased, especially upper incisors inclination (U1/SN, 1+/NA) with improvement of the overjet as result, the lower incisors (L1/MP, 1-/NB) became retroclined, due to, the force exerted by the chin cup of the face mask, also the design of this intraoral appliance depends on positioning the mandible posteriorly which in turn suggested more skeletal than dentoalveolar changes. Previous studies have approved that this backward of the mandible was a major contributing factor in establishing an improvement in anterior overjet.[25] Dentally, the force exerted by the chin cup caused lingual inclination of the mandibular incisors, while the protractive force caused proclination in the maxillary incisors. In the present work, the position of mandibular first molar in relation to the L6-MP and the maxillary first molar in relation to the palatal plane (U6-pp) showed non-significant difference; in contrast with face mask and rapid maxillary expansion therapy because of the elimination of molar extrusion caused by rapid maxillary expansion.[26,27]
CONCLUSION
In the present study, it can be concluded that Wunderer’s activator and a face mask were successful in improving the skeletal and dentoalveolar discrepancy, and it could be used in correction of skeletal Class III due to maxillary deficiency by restricted the growth of the mandible and enhance the advancement of the maxilla.